핵심 개념
이 기사에서는 가장 일반적으로 사용되는 일부 코로나19 약물의 기본 생화학적 기초를 조사합니다. 강력한 SARS-CoV-2 바이러스와 싸우는 데 있어서 이들의 작용 메커니즘, 약동학 원리 및 유용성에 대해 배우게 됩니다. 또한 제약 목표, 증가하는 항바이러스제 내성 문제, 보완적이고 보완적인 코로나19 치료 옵션에 대해서도 알아보게 됩니다.
이 기사는 코로나19를 사례 연구로 삼아 화학과 공중 보건의 교차점을 다룬 ChemTalk 특별 시리즈의 다섯 번째 기사입니다. 이 시리즈를 통해 약물 발견 및 개발 과정, 질병 진단 및 예방에서 화학의 중심 역할, 화학 및 공중 보건의 최전선에 있는 직업에 대해 배울 수 있습니다.
이 미니시리즈의 다른 기사
> 코로나바이러스의 화학
> 약물 발견 과정
> 신약 개발 과정
> 공중 보건 분야의 화학 채용
> 실험실 진단의 질병 탐지 업무
> 질병 예방을 위한 과학적 전략
> 화학, 공중 보건, 그리고 당신
코로나19가 신약 개발 과정에 어떤 영향을 미쳤나요?
지금까지 우리는 제약 공정의 체계적인 단계와 의약품을 만드는 많은 생의학 전문가를 둘러보았습니다. 이는 약물 개발이 어떤 모습인지에 대한 "정상적인" 그림을 나타냅니다. 하지만 팬데믹과 같은 건강 위기 상황에서는 역학적 상황이 급격하게 변하기 때문에 그 상황도 급격하게 변할 수 있습니다.
코로나19에 대한 공중보건의 대응은 많은 변화를 겪었습니다. 특정 도시가 지역적 발병을 길들일 때마다 다른 곳에서 또 다른 발병이 발생했습니다. 전체 산업이 심각한 경제적 영향을 받았고, 일부 산업은 오늘날에도 여전히 회복되고 있습니다. 장기적인 사회적 고립의 결과는 우리가 서로 상호 작용하는 방식을 변화시켰고 일부 사람들의 정신 건강에 영향을 미쳤습니다. 그 동안 의료인들은 의료 인프라가 열악한 상황에서 급증하는 환자를 관리해야 했습니다.
팬데믹이 시작될 때 변경해야 했던 또 다른 구성 요소는 약물 개발 프로세스였습니다. 일반적으로 매우 조직적이고 표준화된 운영이 갑자기 팬데믹의 진화하는 사회적, 경제적, 정치적 지형을 따라잡기 위해 안간힘을 쓰게 되었습니다. 생명의학 연구자들은 코로나19 치료제를 개발하고 테스트하기 위해 공동의 노력을 기울였으며 궁극적으로 코로나19의 원인인 SARS-CoV-2를 정확히 찾아내는 새로운 약물과 백신을 생산하는 데 성공했습니다.
이 글에서는 몇 가지 대표적인 코로나19 약물의 작용 방식과 전반적인 팬데믹 대응에 어떻게 적용되는지에 집중할 것입니다. 지금은 큰 그림의 관점에서 한발 물러나 이 약물이 우리 시대 최악의 건강 위기 중 하나를 막는 데 어떻게 도움이 되었는지에 대한 작은 규모의 세부 사항을 확대해 보겠습니다.
COVID-19 치료제로 항바이러스제를 사용하는 이유는 무엇인가요?
코로나19 의약품은 SARS-CoV-2 바이러스를 표적으로 삼으므로 일종의 항바이러스제입니다. . 다른 병원체에 비해 바이러스는 치료하기가 특히 까다로울 수 있습니다. 그 이유에 대해서는 곧 더 자세히 논의할 것입니다. 엄밀히 말하면 바이러스성 질병을 “치료”하거나 근절할 수는 없지만, 바이러스가 진행되는 동안 증상을 관리할 수는 있습니다. 항바이러스 약물은 대개 신체적 증상을 완화하고 환자가 회복되는 동안 질병이 다른 사람에게 퍼지는 것을 방지하기 위한 것입니다.
항바이러스제는 항생제와 극명한 대조를 이룹니다. , 병원체가 박테리아인 감염을 치료하는 데 사용됩니다. 항생제는 그 자리를 차지하지만, 코로나19는 박테리아가 아닌 바이러스에 의해 발생하기 때문에 결코 현실적인 코로나19 치료 옵션이 아니었습니다. 항생제가 사용하는 박테리아 살해 기술은 바이러스를 퇴치하는 데 아무런 도움이 되지 않습니다. 이는 포크로 수프를 먹으려는 것과 같습니다.
대신, 우리는 바이러스에 맞서 싸울 만한 약을 만들어야 합니다. 항바이러스제를 개발할 때 연구자들은 먼저 특정 바이러스가 어떻게 작용하는지, 즉 바이러스가 신체에 들어가는 방식, 건강한 세포를 감염시키는 방식, 사람 사이에 전파되는 방식 등을 평가합니다. 연구자들은 바이러스의 메커니즘을 이해함으로써 약물의 메커니즘을 결정할 수 있습니다. 약물은 바이러스의 정상적인 기능을 방해하거나 최소화하는 방식으로 작동해야 합니다.
이러한 전략적 접근 방식은 더 광범위한 약물 발견의 초기 단계를 반영합니다. 이 과정을 통해 생의학 과학자들은 약물 설계의 가장 초기 단계를 밟게 됩니다. SARS-CoV-2와 같은 코로나바이러스는 건강한 세포의 분자 생물학 기계를 탈취하여 자신의 유전 물질을 재생산합니다. 이 사실을 알고 연구자들은 바이러스가 숙주 세포에 들어가거나 사용하는 능력을 방해하는 약물을 설계하는 데 노력을 집중했습니다. 이러한 프로세스가 진정될 수 있다면 SARS-CoV-2와 전염병 전체도 진정될 수 있습니다. 따라서 이는 다음으로 중요한 질문을 제기했습니다. SARS-CoV-2의 일반적인 전술을 방해하는 항바이러스 약물을 어떻게 만들 수 있습니까?
이 기사 미니 시리즈의 앞부분에서 일상적인 약물 발견 기술과 두 가지 예시 약물의 기능에 대해 논의했던 것을 기억하실 것입니다. 이 섹션에서는 화학적 관점에서 이러한 인기 있는 코로나19 약물 중 하나와 그 선행 약물의 생성을 다시 살펴보겠습니다. 이 작업은 전염병을 해결하기 위한 과학자들의 접근 방식을 안내했습니다. 생의학 연구자들이 이끄는 제약 실험실은 곧 임무 통제 센터가 되었습니다. 그런데 코로나19 치료제를 개발하기 위해 이 실험실에서 정확히 무슨 일이 일어났나요?
COVID-19 약물 익히기
때는 2020년 초, SARS-CoV-2가 전 세계적으로 활발하게 대혼란을 일으키고 있는 가운데 코로나19 치료제에 대한 검색이 한창입니다. 전 세계 연구팀은 이 괴물을 물리칠 수 있는 약물 후보를 독립적으로 협력하여 개발하고 있습니다. 하지만 그 과정에는 무엇이 수반됩니까? 그리고 구원을 애타게 기다리는 환자들에게는 어떤 의미가 있을까요?
코로나19가 팬데믹으로 확대되자 과학자들은 낭비할 시간이 없다는 것을 깨달았습니다. 환자, 의료 종사자, 기업, 정부 및 일반 대중은 쉽게 배포할 수 있는 안전하고 효과적인 치료법을 개발하기를 기대하고 있었습니다. 질병의 급속한 확산과 그 배경에서 발생하는 공급망 문제를 고려할 때 이러한 약물 특성은 매우 중요했습니다. 오늘날 가장 널리 사용되는 코로나19 약물 중(이러한 기준을 성공적으로 달성한 약물)은 니르마트렐비르/리토나비르라는 항바이러스 약물입니다. . 이 약은 브랜드 이름인 Paxlovid로 더 잘 알 수 있습니다. 생의학 과학자들이 아주 짧은 순간에도 어떻게 이와 같은 코로나19 약품을 개발했는지 간략하게 이야기해 보겠습니다.
모두가 좋아하는 복귀 스토리:코로나19 치료제 제조
이상적인 코로나19 약물의 특성을 방금 확인한 제약 연구원의 입장이 되어 보세요. 다음은 가장 중요한 부분이며 아마도 직면하게 될 가장 큰 장애물입니다. 실제로 어떻게 만들 것인가? 원하는 분자를 생성하기 위해 몇 가지 전구체 물질의 화학적 성질을 어떻게 조작할 수 있습니까? 약물의 효과를 높이는 특성을 이미 결정했으므로 이제 약물 자체를 만드는 과정을 신중하게 고려해야 합니다. 코로나19 치료제로 사용되는 세 가지 화합물의 맥락에서 이를 평가하겠습니다.
니르마트렐비르/리토나비르 및 루포트렐비르
강력한 합성 경로에는 몇 가지 필요한 것이 있습니다. 최고의 합성 접근법은 출발 물질을 거의 사용하지 않고 약물 개발에 드는 재정적 비용을 최소화하는 것입니다. 또한 빠른 반응을 통해 약물 생산 과정을 가속화하여 약물이 환자에게 더 빨리 도달할 수 있도록 합니다. (이 점은 팬데믹이 가장 심한 시기에 코로나19 약물을 만들 때 특히 중요했습니다!) 또한 우리는 가능한 한 부작용을 최소화하여 약물의 순도를 극대화하고 불필요한 낭비를 방지하는 전략을 원합니다. 적은 노력, 높은 수율의 화학 합성은 제약 제조업체의 수익을 향상시키고 궁극적으로 보다 효율적인 의약품 생산으로 이어집니다.
연구자들은 리토나비르(이미 HIV 약물로 존재함)를 코로나19 치료를 위해 용도를 변경한 반면, 니마트렐비르는 처음부터 합성되었습니다. 이는 루포트렐비르라는 또 다른 분자의 후손입니다. , 이는 실제로 코로나19 임상시험에서도 연구된 바 있습니다. 곧 살펴보겠지만, 니마트렐비르와 루포트렐비르의 차이점은 작용 방식(둘 다 프로테아제 억제제)이 아니라 환자의 신체에 전달되는 방식에 있습니다.
팬데믹을 극복하는가? 시아-문제없어요!
약물 개발에는 동일한 최종 제품을 달성하기 위한 여러 가지 수단이 있는 경우가 많습니다. 가장 중요한 것은 최종적으로 생성되는 분자, 그것이 올바른 위치에 올바른 기능 그룹을 갖고 있는지, 그리고 치료 목표를 달성하는지입니다. 원하는 화합물의 분자 구조가 이미 출발 물질에 존재하기 때문에 기존 화합물로부터 새로운 화합물을 합성하는 것은 쉬운 선택인 경향이 있습니다. 니마트렐비르를 만들기 위해 과학자들은 트리펩타이드 사슬의 뼈대부터 시작했습니다.
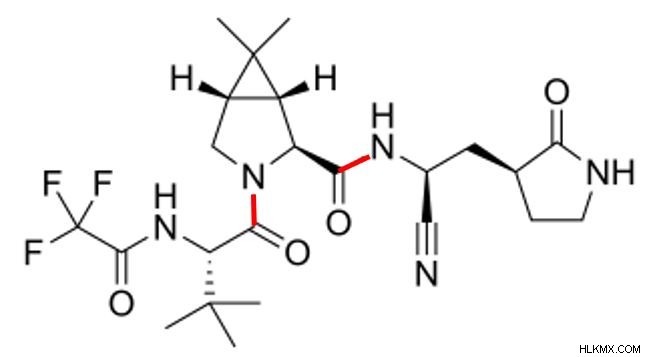 Nirmatrelvir의 화학 구조. 두 개의 펩타이드 결합과 시아노 작용기에 특별한 주의를 기울이십시오.
Nirmatrelvir의 화학 구조. 두 개의 펩타이드 결합과 시아노 작용기에 특별한 주의를 기울이십시오. 이 분자 형태에 대해 이해해야 할 두 가지 중요한 점이 있습니다. 첫째, nirmatrelvir를 자세히 살펴보면 구조 내에서 두 개의 펩타이드 결합을 볼 수 있습니다(위의 빨간색으로 강조 표시됨). 이는 니마트렐비르가 세 개의 펩타이드가 결합되어 구성되어 있다는 단서입니다. 이 경우 문제의 세 가지 펩타이드는 자연에 존재하지 않습니다. 합성 화학자들이 그것을 수정했습니다. 니마트렐비르 합성에는 일련의 축합 반응을 수행하여 펩타이드 결합을 형성하고 단일 분자 내에서 3개의 펩타이드를 결합시키는 작업이 포함됩니다.
nirmatrelvir를 구성하는 펩타이드는 자연에 존재하지 않으므로 nirmatrelvir는 펩티도미메틱입니다. 분자. 펩티도미메틱은 펩타이드와 유사하고 그 기능을 모방하지만 합성이기 때문에 천연 단백질이 나타내는 문제를 우회하는 경우가 많습니다. 문제의 펩타이드 모방 분자에 따라 실제 펩타이드보다 더 나은 안정성, 선택성 또는 효능을 나타낼 수 있습니다. 이러한 모든 요인은 약물이 체내에서 얼마나 오래 지속되는지, 관심 병원체를 얼마나 잘 표적으로 삼는지 등 약물의 효과에 영향을 미칩니다. 따라서 펩티드 모방 약물의 가장 큰 이점은 연구자들이 화학적 합성을 통해 특정 치료 계획의 필요에 맞게 그 작용을 맞춤화할 수 있다는 것입니다. 지속적으로 이동하고 파악하기 어려운 바이러스와 싸울 때 맞춤형 펩티드 모방 약물은 열추적 미사일과 같습니다. 강력하고 정확하며 표적에 고정됩니다.
둘째, 우리는 니마트렐비르가 그 조상인 루포트렐비르에는 없는 특징인 탄소-질소 삼중 결합의 자랑스러운 소유자임을 알 수 있습니다. 에너지가 높고 상대적으로 불안정한 시아노 그룹 이는 nirmatrelvir의 코로나19 약물로서의 기능에 매우 중요합니다. "친전자성 탄두"라고 불리는 이 개체는 주요 프로테아제를 표적으로 삼습니다. (엠프로 ) SARS-CoV-2 복제를 촉진합니다. nirmatrelvir의 시아노 그룹이 Mpro의 시스테인 잔기와 직접 접촉하면 바이러스가 번식하는 데 사용하는 단백질을 만드는 Mpro의 능력을 억제합니다. 코로나바이러스 계열의 구성원 중 Mpro 분자는 고도로 보존되어 있습니다. 이는 바이러스의 수명 주기에서 근본적인 역할을 하기 때문입니다. 그러나 이러한 보존을 통해 nirmatrelvir는 여러 가지 다른 코로나바이러스 변종과 싸울 수 있는 능력을 갖추게 됩니다. 이렇게 작은 원자 쌍이 약물의 기능은 물론 환자의 예후에도 큰 영향을 미친다는 사실은 심오합니다.
버디 시스템:코로나19 퇴치에서 리토나비르의 역할
그러나 니마트렐비르만으로는 이 모든 것을 할 수 없습니다. 이 까다로운 노력을 함께 수행할 때 다른 화합물인 리토나비르의 지원으로 훨씬 더 잘 작동합니다. 환자가 니마트렐비르의 복용량을 섭취한 후에는 (다른 알약과 마찬가지로) 신체 소화 시스템의 대사적 분노를 받게 됩니다. (나중에 자세히 설명합니다!) 지금은 신체의 소화력이 시간이 지남에 따라 알약을 분해한다는 점을 이해해야 합니다. 알약이 빨리 분해될수록 치료 효과의 지속 기간도 짧아집니다.
따라서 니마트렐비르와 같은 코로나19 약물을 장기간 더 효과적으로 만들기 위해서는 신체의 신진대사를 늦추는 방법을 찾아야 합니다. 이것이 바로 리토나비르가 빛을 발하는 부분입니다. 유일한 역할은 nirmatrelvir의 분해를 줄여 nirmatrelvir가 더 오래 작용할 수 있도록 하는 것입니다. 리토나비르는 CYP3A4를 억제합니다. , 약물 대사를 촉매하는 간에서 풍부하게 발견되는 시토크롬입니다. 분해가 억제된 nirmatrelvir는 이제 일반적으로 이를 대사하는 효소를 성공적으로 피할 수 있습니다. 이를 통해 환자는 리토나비르가 없는 경우보다 더 오랫동안 니마트렐비르의 치료 효과를 경험할 수 있습니다.
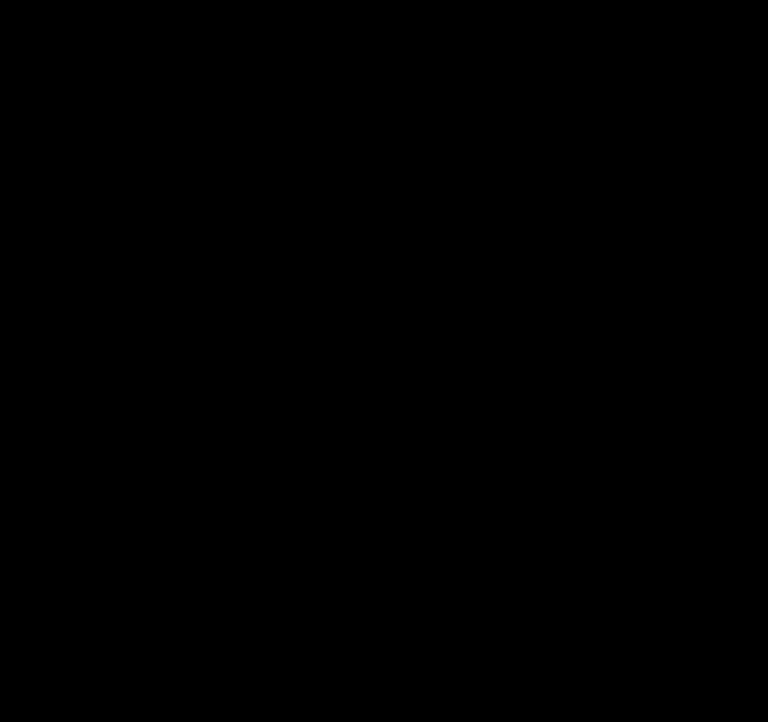 리토나비르 분자. 이 이미지 상단 근처에 두 개의 티아졸 고리가 있습니다.
리토나비르 분자. 이 이미지 상단 근처에 두 개의 티아졸 고리가 있습니다. CYP3A4를 억제할 수 있는 리토나비르 구조의 특별한 점은 무엇입니까? 두 개의 티아졸 그룹입니다! 티아졸 그룹은 5개의 원자(질소와 황 포함)와 2개의 이중 결합을 가진 헤테로사이클릭 고리입니다. 리토나비르에서 이러한 티아졸 그룹은 두 가지 매우 중요한 방식으로 약물을 지원함으로써 이중 임무를 수행합니다. 구조적 관점에서 볼 때 각 고리는 리토나비르의 다른 대부분의 구성 요소보다 훨씬 큽니다. 분자의 양쪽 끝에 티아졸 그룹을 배치하면 리토나비르의 전반적인 안정성이 증가하여 구조가 더욱 견고해집니다.
티아졸 그룹의 또 다른 중요한 목적은 리토나비르가 CYP3A4와 상호작용하는 곳이라는 것입니다. CYP3A4에는 헴이 포함되어 있습니다. 철 원자를 가지고 있는 그룹. 리토나비르의 티아졸 그룹에 있는 질소는 이 철 원자와 밀접하게 결합하여 높은 결합 친화력으로 선택적 상호 작용을 유도합니다. 사실 이 결합은 너무 강력해서 되돌릴 수 없습니다. 즉, 신체는 결국 리토나비르와 니마트렐비르 분자를 필연적으로 대사하게 됩니다. 그럼에도 불구하고, 이 매우 구체적이고 되돌릴 수 없는 결합 작용은 약물의 효과가 그런 일이 발생하기 전에 최대한 오래 지속되도록 보장합니다.
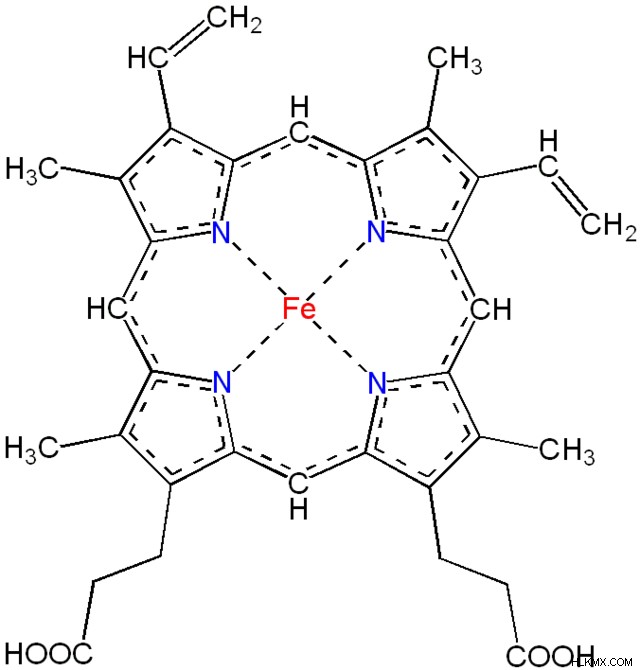 철 원자(빨간색)와 비편재화된 전자(점선)를 보여주는 헴 그룹 구조의 개요입니다. 리토나비르의 티아졸 그룹은 철분과 결합하여 CYP3A4의 대사 활동을 억제합니다.
철 원자(빨간색)와 비편재화된 전자(점선)를 보여주는 헴 그룹 구조의 개요입니다. 리토나비르의 티아졸 그룹은 철분과 결합하여 CYP3A4의 대사 활동을 억제합니다. 변화 수용:전구약물이 활성 형태로 전환되는 방법
이제 니마트렐비르의 전신인 루포트렐비르에 대해 다시 살펴보겠습니다. 루포트렐비르가 혈류에 도달하면 알칼리성 포스파타제 효소가 생성됩니다. 상당히 빠르게 활성 형태로 분해됩니다. 따라서 루포트렐비르 자체는 전구약물입니다. , 생체 내에서 활성 형태로 전환되는 약물 활성 형태의 비활성 전구체 . 약물의 활성 형태인 이 절단된 루포트렐비르 버전은 항바이러스 기능을 가지고 있습니다. 이것이 코로나19 치료제로서의 성공의 핵심이다. 다행스럽게도 루포트렐비르는 다양한 변종에도 불구하고 효과를 보여주었습니다. 이는 SARS-CoV-2 바이러스가 돌연변이하는 것을 여러 번 목격했기 때문에 귀중한 특성입니다.
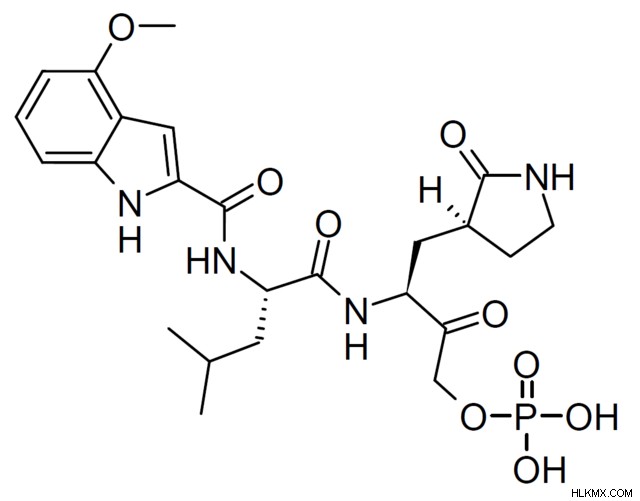 루포트렐비르의 분자 구조. 우리는 nirmatrelvir가 시아노 그룹을 가지고 있는 곳에 인산염 그룹이 존재한다는 것을 알 수 있습니다.
루포트렐비르의 분자 구조. 우리는 nirmatrelvir가 시아노 그룹을 가지고 있는 곳에 인산염 그룹이 존재한다는 것을 알 수 있습니다. 원래 lufotrelvir는 에피머화되는 경향이 있기 때문에 안정성이 부족했습니다. 에피머 간 상호 변환 (하나의 다른 키랄 중심을 갖는 부분입체이성질체)은 분자의 생체활성, 신진대사 및 분해에 저항하는 능력에 영향을 미칠 수 있습니다. 루포트렐비르의 경우 분해 경향이 특히 두드러진 문제였습니다. 이 문제를 해결하기 위해 제약 과학자들은 약물 개발 과정에서 루포트렐비르를 변형했습니다. 이러한 변형에는 Claisen 첨가(탄소-탄소 결합을 형성하여 분자를 확장) 및 인산화(인산염 그룹 생성)가 포함됩니다. 분명히 이러한 변화는 그만한 가치가 있었습니다. 임상 연구에 따르면 전구약물은 거의 완성되어 활성 형태로 전환됩니다. 약물의 활성 비율이 높을수록 약물을 탄생시키는 데 드는 비용과 시간이 많이 소요되는 약물 개발 노력을 최대한 활용하기 때문에 약물의 효율성이 더욱 높아집니다.
루포트렐비르가 혈류에서 활성 형태로 분해되는 것을 기억하십시오. 이는 루포트렐비르가 정맥 내로 직접 혈류로 투여된다는 사실에 의해 촉진됩니다. 루포트렐비르의 활성 형태가 효과를 발휘한 후 신체는 아미드 가수분해를 통해 약물을 제거합니다. 이 대사 과정은 곧 더 자세히 살펴보게 될 것입니다. 지금까지 우리는 코로나19 약물이 체내에 들어가면 어떤 역할을 하는지에 대해 많은 것을 배웠습니다. 다음으로, 한 걸음 물러서서 우리가 언급했던 주제, 즉 애초에 약물이 몸에 어떻게 들어가는지 살펴보겠습니다.
약물 전달의 복잡성
Nirmatrelvir와 그 전구체 분자인 lufotrelvir는 밀접하게 관련되어 있지만 상당한 차이점이 있습니다. 이 두 가지 약물 중에서 니마트렐비르(리토나비르 화합물과 함께 사용되는 경우)는 알약으로 투여할 수 있기 때문에 일반적으로 선호되는 치료 옵션입니다. 반면, 루포트렐비르는 정맥 주사로만 투여할 수 있어 덜 편리한 대안입니다.
환자가 약물을 어떻게 소비하는지가 중요합니다. 알약은 휴대가 가능하고 이미 적절한 용량으로 나누어져 있으며, 환자가 의료 서비스 제공자(HCP) 없이도 각 용량을 복용할 수 있기 때문에 환자에게 편리합니다. 편의성은 환자의 관점뿐만 아니라 HCP의 관점에서도 약물 치료에 있어서 매우 바람직한 특징입니다. 환자는 약을 계속 복용하고, 편리하다면 처방된 대로 정확히 복용할 가능성이 훨씬 더 높습니다. 결국, 환자가 해당 약을 적절하게 사용하지 않고 그 효과로부터 이익을 얻지 못한다면 약을 처방하는 것은 환자에게도, 의료 서비스 제공자의 시간을 들일 가치도 없습니다.
알약의 가장 큰 단점은 효과가 나타나는 데 걸리는 시간입니다. 알약을 경구로 섭취하면 소화 시스템을 통과합니다. 위산이 이를 분해한 다음 장에서 흡수합니다. 이 과정은 환자의 입장에서는 쉽지만 시간이 걸립니다. 부산물로서 약물의 화합물을 생화학적 분해에 적용하기도 합니다. 방법을 살펴보겠습니다.
생체 이용률 및 약물 안정성
소화 시스템의 모든 단계에서 이러한 화합물은 효소와 같은 소화제와 만나 상호 작용합니다. 화학 반응과 대사 기능을 통해 이러한 효소는 화합물의 화학 구조에 대한 기능 그룹을 변형하여 생물 의학 연구자가 의도한 것에서 벗어날 수 있습니다. 신체가 약물을 흡수하기 전에 이런 일이 발생하면 약물의 전반적인 효과가 떨어집니다. (음식과 함께 또는 음식 없이 약을 복용하라는 지시를 받은 적이 있다면 이것이 그 이유 중 하나입니다! 음식이 위에 있는지 여부에 따라 신체가 일부 약물을 더 효과적으로 또는 덜 효과적으로 흡수할 수 있습니다.) 건강 관리 맥락으로 전환하면 이러한 상황으로 인해 환자가 치료상의 이점을 덜 경험하게 될 수 있습니다.
반대로, 정맥 주사 약물은 혈류로 직접 전달되며, 그 효과는 알약보다 훨씬 빠르게 나타납니다. 모든 정맥 주사 약물은 소화 과정을 완전히 건너뛰기 때문에 완전한 생체 이용률을 보여줍니다. 생체 이용 가능성 순환계에 도달하는 약물의 비율을 측정하므로 정맥 주사 약물의 (이론적) 생체 이용률은 100%입니다. 알약은 소화 과정으로 인해 약물의 일부가 항상 신체의 신진대사로 손실되기 때문에 생체 이용률이 낮습니다. 과학자들은 약물의 지속 기간을 나타내는 지표로 생체 이용률을 측정합니다. 생체 이용률이 높을수록 환자는 생체 이용률이 낮은 약물에 비해 단일 용량의 효과가 더 오래 지속되는 것을 느낄 것입니다. 따라서 약물 투여 방법에 따라 환자가 약물을 경험하는 방식과 기간이 달라집니다. 생체 이용률과 같은 표준화된 측정을 사용하면 연구자들이 매우 다양한 약물을 공정하게 비교할 수 있어 대화가 더욱 활발해집니다.
약물이 알약과 정맥 주사 형식으로 모두 제공되는 경우 각 형식은 서로 다른 복용량을 사용합니다. 이는 형식의 생물학적 이용 가능성의 차이를 보상합니다. 이제 우리는 약이 알약일 때 순환계에 도달하는 약의 양이 더 적다는 것을 알고 있습니다. 약물이 알약으로 전달되는 경우 정맥 내로 전달되는 경우에 비해 더 높은 용량으로 전달됩니다. 생체 이용률은 약물의 전달 형식, 복용량 수준, 투여와 같은 요인과 직접적인 관련이 있다는 것이 여기서 분명합니다.
또한 다른 미묘한 요인도 작용한다는 점을 명심하십시오. 예를 들어, 환자 집단 내에서 연구자들은 각 환자가 약물을 흡수하는 속도와 양에 대한 개인차를 확인합니다. 연구자들은 약물 흡수가 약물 복용 시간, 환자의 체중, 생물학적 성별 등과 같은 요소에 따라 달라진다는 것을 어느 정도 이해하고 있습니다. 그러나 약물을 설계할 때 연구자들은 흡수에 영향을 미칠 수 있는 모든 다양한 특성을 완전히 설명할 수 없습니다. 대신 그들은 안전하고 예측 가능하며 최대한 효과적인 방식으로 대다수의 환자에게 효과가 있는 약품을 설계하기 위해 노력합니다.
이러한 모든 고려 사항은 약물 안정성을 둘러싼 대화를 풍성하게 합니다. 의약품에서는 안정성 의약품이 제조된 시점부터 환자가 사용하는 시점까지 일관된 특성을 유지하는 약물의 능력을 말합니다. 약물의 안정성 평가는 환자의 신체 내부와 외부에서 지속적으로 이루어집니다. 예를 들어, 제약 연구자들은 약품이 유통기한에 안정적이고, 유효기간까지 품질과 효과를 안정적으로 유지하며, 복용 후 환자의 건강에 의미 있는 영향을 미치기를 원합니다. 안정성이 낮다는 것은 약물이 의도한 만큼 오랫동안 의도한 대로 효과가 없다는 것을 의미합니다. 이는 분명히 자신의 약물이 제대로 작동할 것으로 기대하는 환자에게 심각한 결과를 초래할 수 있습니다.
산화와 가수분해의 다가오는 위협
일상적으로 약물 안정성을 위협하는 화학 반응의 두 가지 예는 산화와 가수분해입니다. 산화 전자가 손실되는 반응은 약물을 빛이나 열과 같은 조건에 노출시킴으로써 시간이 지남에 따라 발생할 수 있습니다. 분해를 방지하기 위해 제조업체는 온도 범위, 빛으로부터 얼마나 보호되는지 등 약물 보관에 대한 구체적인 지침을 제공합니다. 화합물이 다른 분자의 전자를 훔치고, 교환하고, 잃거나 얻는 방법에 따라 얼마나 많은 화학 반응이 달라지는지 생각해 보십시오. 잘못된 보관 조건으로 인해 조기에 산화가 발생하면 약물의 화학 구조에 필요한 전자 수가 달라져 일반적인 방식으로 이러한 반응을 겪지 않게 됩니다. 어떤 경우에는 이로 인해 약물 자체가 제대로 작동하지 않을 수도 있습니다.
의약품 제조업체의 보관 지침을 준수하는 것만으로도 산화 가능성을 최소화할 수 있습니다. 그러나 산화 외에도 약물 분해에 대해 더 일반적으로 관찰되는 경로는 가수분해입니다. 가수분해 분자의 화학 결합을 끊기 위해 물을 사용하는 것과 관련이 있습니다. 분자의 시작 구조에 따라 간단한 가수분해 반응으로 생화학적 프로필이 완전히 바뀔 수 있습니다. 물이 존재하면 의약품에서 자주 발견되는 작용기(예:에스테르와 아미드)가 카르복실산이나 알코올기로 전환될 수 있습니다.
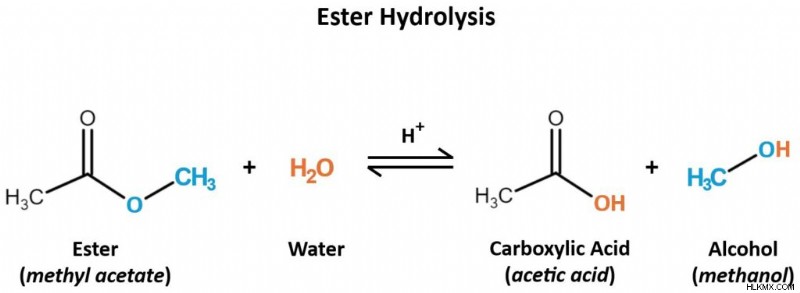 산성 조건에서 물 분자는 에스테르 분자를 카르복실산과 알코올 산물로 가수분해합니다. 이는 가역적인 반응이지만 약물의 기능을 방해할 가능성이 있습니다.
산성 조건에서 물 분자는 에스테르 분자를 카르복실산과 알코올 산물로 가수분해합니다. 이는 가역적인 반응이지만 약물의 기능을 방해할 가능성이 있습니다. 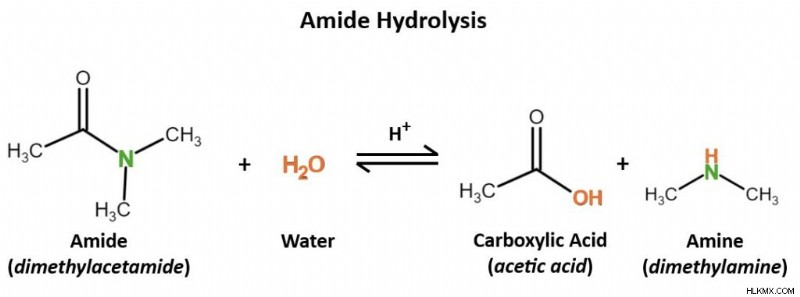 물은 다시 산성 조건에서 아미드를 가수분해하여 카르복실산과 아민 생성물을 생성합니다.
물은 다시 산성 조건에서 아미드를 가수분해하여 카르복실산과 아민 생성물을 생성합니다. 신체 내에서 가수분해는 다양한 조직에서 발견되는 효소 덕분에 일어납니다. 이러한 효소가 약물을 더 빠르게 가수분해할수록 해당 약물의 효과가 지속되는 시간도 짧아집니다. 가수분해되지 않은 약물과 동일한 이점을 얻으려면 더 자주 또는 더 많은 용량을 투여해야 할 수도 있습니다. 따라서 약물의 효과를 높이는 한 가지 방법은 애초에 가수분해되기 쉬운 작용기를 사용하여 약물을 설계하는 것입니다.
그럼에도 불구하고 약물이 화학 반응을 겪는다는 사실이 본질적으로 나쁜 것은 아닙니다. 결국, 약물은 결국 분해되어야 합니다! 그렇지 않으면 약물 수치가 체내에 지속적으로 축적되어 환자는 독성이나 장기 손상과 같은 불쾌한 부작용을 겪을 수 있습니다. 중요한 것은 연구자들이 약물 대사의 미묘한 균형을 어떻게 맞추느냐입니다. 이상적으로, 약물은 환자의 신체에서 치료 효과를 가질 수 있을 만큼 충분히 오랫동안 조기 화학 반응에 저항해야 합니다. 이러한 효과가 완료된 후에는 대사 화학 반응에 굴복하여 신체가 이를 배설할 수 있습니다. 이러한 대사가 언제 일어나야 하는지를 정확히 찾아내는 것은 연구자들이 생체 내 약물을 연구하는 약물 개발 단계에서 핵심적인 질문입니다. 신체의 활성 효소, 화합물 및 조직에서 이것이 어떻게 기능하는지 이해합니다.
이 글에서 소개한 각 코로나19 약물은 고유한 특성과 관계없이 항바이러스제 역할을 합니다. (잠깐만: 확실히 구별하는 방법은 각 이름 전체에 "-vir"로 끝나는 것입니다.) 그러나 이 네 가지 화합물 중 하나는 다른 화합물과 다릅니다. 리토나비르는 단순한 항바이러스제가 아닙니다. 항레트로바이러스제입니다 . 코로나19 상황에서 이것이 무엇을 의미하는지 생각해 봅시다.
백업:레트로바이러스란 무엇인가요?
항바이러스 약물은 하나 이상의 바이러스를 표적으로 삼지만, 항레트로바이러스 약물은 특히 레트로바이러스를 표적으로 삼습니다. . 숙주 세포를 감염시키면 레트로바이러스는 역전사효소를 사용합니다. 자신의 RNA 게놈에 상보적인 DNA 가닥을 생성하는 효소. 생물학의 중심 교리는 DNA가 RNA로 전사되어 결국 단백질을 만든다는 것을 기억하십시오. RNA로부터 DNA를 만든다는 것은 일반적인 전사 과정을 역전시키는 것을 의미합니다. 이 RNA-to-DNA 서열은 레트로바이러스가 그 이름을 얻은 곳입니다. 유전 물질이 DNA로 변환되면 레트로바이러스는 숙주 세포의 자연 복제 기계를 대신할 수 있습니다. 이를 통해 레트로바이러스는 게놈을 복제하고 새로운 복사본을 만들어 감염을 전파할 수 있습니다. 아마도 레트로바이러스의 가장 잘 알려진 예는 HIV/AIDS의 원인이 되는 바이러스인 HIV-1일 것입니다.
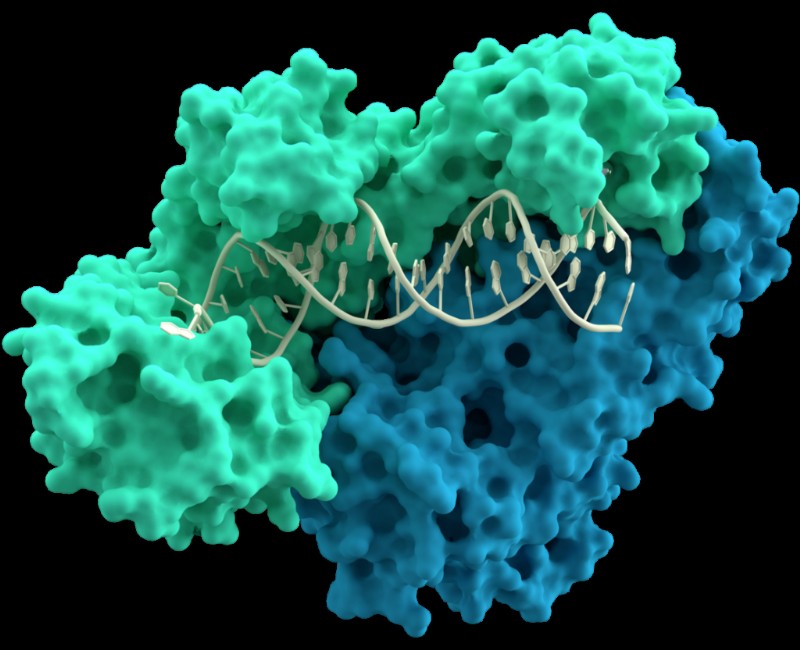 DNA 분자와 상호작용하는 역전사효소의 p66(녹색) 및 p51(파란색) 하위 단위 모델(가운데).
DNA 분자와 상호작용하는 역전사효소의 p66(녹색) 및 p51(파란색) 하위 단위 모델(가운데). SARS-CoV-2와 같은 코로나바이러스는 레트로바이러스가 아니라는 점에 유의하는 것이 중요합니다. 코로나바이러스와 레트로바이러스는 완전히 다른 분류군에 속합니다. 그렇다면 리토나비르와 같은 항레트로바이러스 화합물이 코로나바이러스 퇴치에 왜 유용할까요?
차이점에도 불구하고 레트로바이러스와 코로나바이러스 사이에는 몇 가지 의미 있는 유사점이 있습니다. 둘 다 RNA를 유전 물질로 사용하고, 숙주 세포의 타고난 메커니즘을 탈취하여 스스로 복제하며, 복제를 위해서는 프로테아제가 필요합니다. 프로테아제 단백질을 분해하는 효소이다. 이 경우 레트로바이러스나 코로나바이러스가 번식하는 데 필요한 단백질을 분해합니다.
Nirmatrelvir와 ritonavir는 물론 lufotrelvir도 모두 단백질분해효소 억제제입니다. . 이들의 목적은 레트로바이러스와 코로나바이러스의 확산을 돕는 프로테아제 효소를 막는 것입니다. 리토나비르는 실제로 HIV-1 치료제로 시작되었습니다. 코로나19 팬데믹 기간 동안 과학자들은 SARS-CoV-2에 대한 영향을 연구하기 위해 리토나비르의 용도를 변경했습니다. 그리고, 그게 영향을 미쳤나요?
신체는 시간이 지남에 따라 특히 장과 간에서 자연적으로 프로테아제 억제제를 대사합니다. 제약학적 관점에서 볼 때 이는 프로테아제 억제제가 필연적으로 분해된다는 것을 의미합니다. 이러한 약물이 체내에서 더 오래 지속되도록 하려면 이 신진대사를 늦추는 다른 약물을 투여할 수 있습니다. 팍슬로비드의 주인공인 니르마트렐비르가 단일약물로 리토나비르를 동반하는 이유다. 둘 다 프로테아제 억제제이지만 리토나비르는 프로테아제 억제제를 분해하는 CYP3A4 효소를 억제하기 위해 특별히 제조되었습니다. 즉, 리토나비르는 니마트렐비르를 대사하는 힘을 늦추어 니마트렐비르가 신체에 더 오랫동안 영향을 미칠 수 있도록 합니다. 신진대사의 위협이 줄어들면서 니마트렐비르는 자신이 가장 잘하는 일, 즉 코로나19 확산을 가능하게 하는 단백질을 분해하는 데 집중할 수 있습니다.
약물의 용도 변경은 시행착오를 겪는 경향이 있습니다. 연구자들은 관심 질병에 대해 이미 알고 있는 정보를 사용하여 어떤 기존 약물이 해당 질병에 효과가 있을지 예측합니다. 그런 다음 실험실 환경과 임상 실험을 통해 해당 약물이 실제로 얼마나 효과가 있는지 테스트합니다. 관심 있는 질병에 대해 작용합니다. 임상시험이 성공하면 규제 당국은 해당 질병을 치료하기 위한 약품을 승인할 수도 있습니다.
약물이 그렇지 않은 경우 일?
약물이 시장에 출시되면 실험실이나 임상 연구 환경을 넘어서 실제로 얼마나 효과가 있는지 확인하게 됩니다. 때로는 약이 단 한 번의 문제 없이 의도한 대로 정확하게 작동하는 경우도 있습니다. 하지만 상황이 계획대로 진행되지 않고 약물이 실제 환자에게 도달한 후에야 새로운 장애물이 드러나는 경우도 있습니다.
우리 시대의 가장 큰 의학적 위협 중 하나인 항생제 내성의 관점에서 이를 살펴보겠습니다. 저항 이는 약물이 표적으로 삼는 병원체(이 경우 질병을 일으키는 박테리아)가 점차적으로 해당 약물(항생제)을 견딜 수 있는 능력이 커진다는 것을 의미합니다. This has dire implications for the pharmaceutical industry, which then must devise a new bacteria-killing drug that the bacteria aren’t resistant to yet, and for the patients who suffer from incurable bacterial infections in the meantime.
Unfortunately, this phenomenon happens with protease inhibitors, too. Viruses that are normally susceptible to protease inhibitors can, over time, develop resistance to those drugs. When that happens, the protease inhibitors become less effective as antiviral medications. How does this happen in the first place?
In order to stop viral replication, a protease inhibitor must bind to a specific site on the virus’s protease. This is how protease inhibitors work under normal circumstances, as intended, to treat a viral infection. In its genome, a virus encodes the proteases that it needs for replication. But, as we know, genetic material can mutate — and any mutation can change the nature of the protease.
If a mutation changes the protease’s active site, this directly impacts its affinity for binding to the protease inhibitor. It’s possible for the active site to mutate to have a lower affinity for the drug, which limits the medication’s ability to target the protease. This is how protease inhibitor resistance arises. Without a selective target available, the protease inhibitor can’t do its job effectively, so it’s no longer a useful solution against the virus it ought to fight.
Mutations can happen spontaneously, and they tend to arise as a virus evolves over many replication cycles. This introduces a bit of a conundrum:scientists invented protease inhibitors to prevent viral reproduction, but as a result of viral reproduction itself, mutations can arise that change a protease inhibitor’s effectiveness. During the COVID-19 pandemic, we saw precisely how concerning viral evolution and mutation are, as newly-evolved mutant variants repeatedly rendered our vaccines less effective.
To overcome the challenging prospect of a protease-inhibitor–resistant virus, protease inhibitors can be used in combination with antiviral medications that have different targets. This way, even if the virus’s active site mutates to become resistant and the protease inhibitor can no longer bind there, another medication can step in to target a different structure or function of the virus instead. Spreading the virus-fighting burden across multiple diverse drug classes can help stop the virus’s spread. But wait — what’s a drug class, and what does it mean for the virus that causes COVID-19?
Class is in Session:Pinpointing the Right Medication for the Right Job
There’s no “miracle” antiviral drug that can treat every viral disease out there, but that doesn’t stop scientists from trying! Researchers group similar medications into classes based on their properties and functions. Oftentimes, these classes directly describe how the drug functions. Some familiar examples readily come to mind:drugs in the stimulant class stimulate the body or mind, contrasted with drugs of the depressant class that reduce arousal, while analgesic drugs relieve pain (the word “analgesic” comes from Greek roots that mean “without pain”).
Protease inhibitors are another class of drugs that do exactly what their name implies. By inhibiting proteases, a type of enzyme that SARS-CoV-2 particles use for reproduction, protease inhibitors interrupt the viral life cycle by preventing the virus from replicating. The virus must make many copies of itself to infect new host cells, so preventing viral replication prevents the spread of COVID-19.
Researchers already applied the same concept to fighting the viruses behind HIV/AIDS and hepatitis C. Understanding the commonalities within a particular drug class makes it easy to translate existing medications into new contexts to treat different diseases. To devise an effective antiviral medication to treat COVID-19, researchers had to understand a few simple, yet essential, points. First, they learned that the SARS-CoV-2 virus uses proteases in its replication process. Second, they knew that the viruses that cause AIDS and hepatitis C also use proteases to reproduce. Third, protease inhibitors already existed as safe, effective medications for treating HIV/AIDS and hepatitis C.
From here, scientists could apply this logic in a straightforward way in order to conclude that protease inhibitors are a viable COVID-19 treatment option. If protease inhibitor drugs are already known to work against other viruses that replicate via proteases, and SARS-CoV-2 is known to replicate via proteases too, why not pursue a protease inhibitor as a COVID-19 drug?
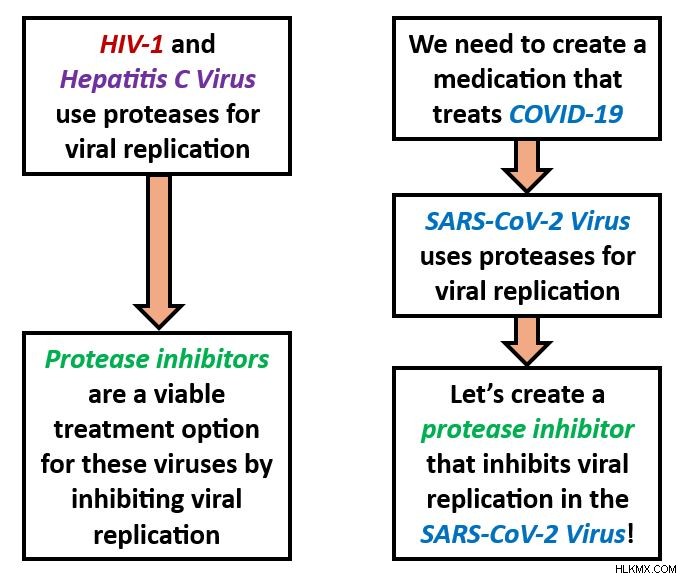 During drug discovery, biomedical researchers don’t always have to start from scratch. Instead, they may be able to build upon existing knowledge of which medications work well against pathogens of similar diseases. Inspired by existing drugs for HIV and hepatitis C, these logical reflections guided researchers to develop protease inhibitors for SARS-CoV-2.
During drug discovery, biomedical researchers don’t always have to start from scratch. Instead, they may be able to build upon existing knowledge of which medications work well against pathogens of similar diseases. Inspired by existing drugs for HIV and hepatitis C, these logical reflections guided researchers to develop protease inhibitors for SARS-CoV-2. In some ways, drug discovery is a very sensible process. But in practice, there are a lot of factors that threaten to get impede what ought to be a smooth, uncomplicated approach. Let’s take a look.
Challenges in Treating COVID-19
Pandemics are among the most urgent public health scenarios; time is truly of the essence. To conquer the crisis, medical experts must develop and distribute a cure faster than the disease is spreading. But we know the SARS-CoV-2 virus causes COVID-19, and viral diseases, in general, cannot be cured — only managed or treated.
Facing an incurable disease, how can we devise an effective treatment, and fast? Taking on this challenge meant overcoming SARS-CoV-2’s natural evasive characteristics, drug development roadblocks, and sociocultural factors that shaped how people interacted with COVID-19. To understand why these details had such a key impact on the pandemic, let’s evaluate them in greater depth.
Virology 101:How Viruses Evade Our Efforts to Eradicate Them
We know how to take control of stubborn viruses because we’ve managed to do it many times before. For example, you’ve likely sustained a barrage of vaccines for viral diseases like chickenpox, measles, and polio. And everyone can recite by heart the cardinal rules of flu season — stay home when you’re sick, cover your mouth when you cough and sneeze, and wash your hands often. Public health principles like these are somewhat of a tradition, and we know these rules of how to beat disease. So, what happens when we encounter a virus that doesn’t play by the rules?
What makes an effective antiviral medication?
Viruses have certain properties that can make them more difficult to target than pathogens like bacteria or parasites. First of all, there’s an ongoing scientific debate as to whether viruses are living or nonliving. Viruses have their own genetic material and, inside of a host cell, they exhibit some characteristics of life, like the ability to reproduce (viral replication ). However, viruses can’t function independently, and therefore can’t do much damage, without the help of a living host cell. Since they need living hosts’ support to execute their functions, many scientists view viruses, in and of themselves, as nonliving. This invites a unique conundrum:If something isn’t alive, is it actually possible to use medications to kill it?
As part of the drug discovery process, pharmaceutical researchers determine how their medication will impact its target (which might be a protein, antibody, gene, virus, bacterium, etc.). Many drugs work by impacting the target’s ability to function, but this might not be useful against viruses. For example, a drug that works by interfering with the target’s metabolism wouldn’t be an effective antiviral drug because viruses don’t have their own metabolic processes.
Living or not, we know that viruses are vulnerable to antiviral medications. Strong antiviral medications account for their target’s normal mechanisms and viral load. By closely studying those mechanisms — how the virus infects and moves through the body, infects healthy host cells, replicates its genetic material, and causes physical symptoms — scientists can pursue a drug that interferes with them.
Viral load refers to how much virus is present in a patient’s blood. Viral load can change over the course of an infection, and it can indicate how sick the patient is. For certain diseases, a higher viral load indicates that the patient is more contagious. Some antiviral medications are intended to reduce viral load, alleviating the patient’s infection and protecting other people from catching it. (In this way, reducing viral load is a goal of a long-term HIV treatment called antiretroviral therapy , or ART .)
What’s the Password?:How Viruses Enter Host Cells
Viruses are among the smallest biological agents. After all, they have to be, in order to penetrate host cells. Viruses usually enter host cells through receptor-mediated endocytosis , a process by which the viral particle binds to a receptor on the cell membrane and passes into the cell. When descending upon a new host cell, the virus hunts for specific receptors that will bind to proteins on its own membrane.
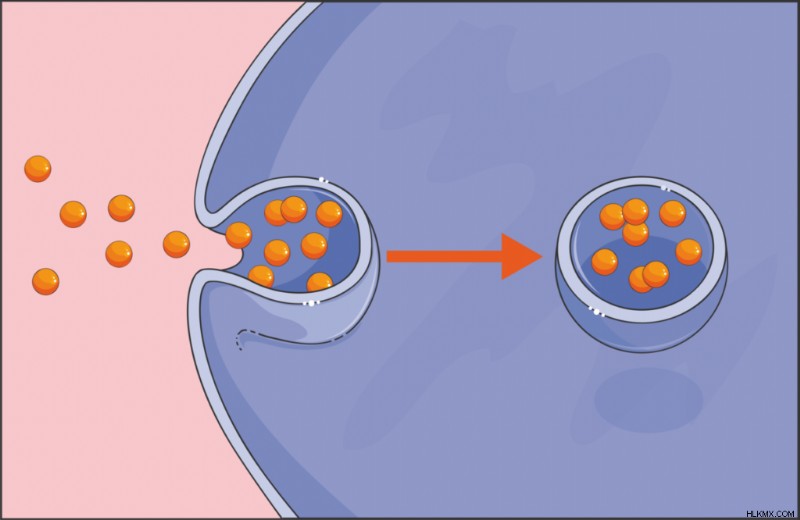 Endocytosis is a process by which particles can enter a cell. Viruses use this tactic to bind to a host cell’s membrane and invade the cell.
Endocytosis is a process by which particles can enter a cell. Viruses use this tactic to bind to a host cell’s membrane and invade the cell. This penetrative mechanism is sometimes what an antiviral drug targets. A drug that interferes with this protein’s binding to a membrane receptor prevents the virus from reaching host cells. Researchers extended this strategy to COVID-19 vaccines that notably target SARS-CoV-2’s spike protein , which binds to host cells’ ACE2 receptors. All coronaviruses have spike proteins, but the protein’s chemical makeup can fluctuate across different viral variants. This is why scientists continuously produced COVID-19 vaccines:each new version of the vaccine targeted the spike protein’s latest disguise. We already knew about coronaviruses before COVID-19 happened, but developing a COVID-19 medication required learning about the special intricacies of SARS-CoV-2’s spike protein in particular.
For being such tiny agents, viruses sure put up a big fight. A drug spurs the body to act upon a virus, but this could inadvertently lay the groundwork for further harm. In order to damage viruses, antiviral treatments must also damage the host cells that those viruses occupy. This can have further implications for the health of the patient or the symptoms that they experience. Therefore, antiviral treatments represent a balancing act, selective toxicity , between destroying the virus and preserving the patient’s own tissues.
Unfortunately, there’s no easy solution to this dilemma. Any step in the viral life cycle would be a good target for an antiviral drug, but the host cell would probably also suffer. Some antivirals reduce the risk to the patient’s health by targeting a virus-specific molecule or behavior, leaving the host cells relatively untouched. That’s the inspiration behind COVID-19 drugs like nirmatrelvir/ritonavir. Nirmatrelvir/ritonavir inhibits a protease that SARS-CoV-2 uses for replication, which prevents the virus from reproducing. (Other COVID-19 medications, like remdesivir , disrupt the replication process by introducing steric hindrance as the virus replicates its RNA. This steric hindrance stands in the way of RNA replicating to completion, putting a pause in the viral life cycle and the SARS-CoV-2 virus at a loss.)
With antiviral drugs, researchers must weigh the benefit of weakening the virus against the risk of weakening host cells. An antiviral medication that preserves a patient’s infected cells would be an ingenious discovery and a very promising treatment option — something to consider next time you find yourself bored in the lab!
Playing the Long Game
Recall from our previous article that public health professionals use epidemiological surveillance to track disease outbreaks on a population scale. We can extend this concept to a much smaller scale:detecting microscopic viruses within the body. Their minute size isn’t the only characteristic that can make viruses hard to detect. Some viruses are pros at staying inconspicuous for extended periods of time. During these periods, the virus in question may not cause obvious symptoms (or if so, the symptoms may be nonspecific). It may even fail to appear on test results.
Sometimes observed in viral infections like HIV, Epstein-Barr virus, and hepatitis, this phenomenon is a latency period. Latency periods happen when the virus is dormant for spans of weeks, months, years, or even decades. Dormancy means that the virus has infected a host, but isn’t actively replicating, or it’s replicating very slowly. Remember, for the infection to spread within the body, or from an infected to healthy person, the virus must replicate. The act of replication kills the host cell. Then, in the aftermath of cell death, the progeny from that replication seek new host cells and spread the infection.
Although certain viruses share some resemblances, like these particular viruses’ ability to stay surreptitious for long-term periods, viruses overall demonstrate very diverse features. For instance, SARS-CoV-2’s genome is composed of RNA, but many viruses’ genomes are made from DNA just like ours. Different viruses also boast different physical properties, replication techniques, and thrive in a range of environmental conditions. Maybe you can’t disrupt the virus’s life cycle, but can you do something to make its environmental conditions less hospitable? In light of such diverse traits, making antiviral medicines might seem like a fruitless pursuit, but keep in mind that every new trait presents a new angle to attach the virus.
Identifying a given virus’s individual idiosyncrasies helps researchers tailor a medication perfectly to that virus — but also means that most antiviral medications can only treat one or a handful of viruses. This lies in stark contrast to broad-spectrum antibiotics , which target numerous bacterial species. Not all antibiotics are broad-spectrum, but this all-encompassing quality is hard to replicate in antiviral drugs. Broad-spectrum antivirals do exist, but because viruses evolve so rapidly, the best antivirals would be able to defeat multiple existing strains while anticipating future variants, which is essentially a guessing game. A good place to start is with antivirals that target entire families of viruses, like coronaviruses or herpesviruses for example, that attack a stable characteristic which all of the family members have in common. Yet another example of how the shared features among different pathogens serve as the groundwork for building a single drug that fights all of them!
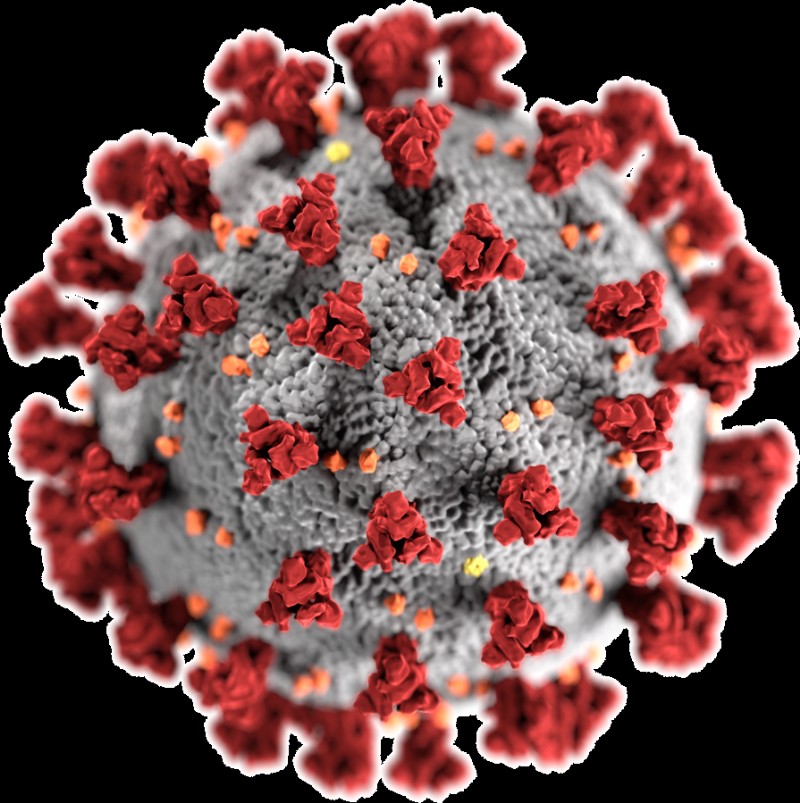 Spike proteins (red) on a SARS-CoV-2 particle project outward to readily bind with ACE2 receptors on a host cell’s membrane.
Spike proteins (red) on a SARS-CoV-2 particle project outward to readily bind with ACE2 receptors on a host cell’s membrane. Ready, Aim, Fire! All about Drug Targets
Earlier, we discussed how protease inhibitors bind with proteases that the SARS-CoV-2, HIV-1, and hepatitis C viruses encode. Recall that this binding happens selectively, and directly leads to the inhibition of viral replication. In pharmaceutical terms, we describe this dynamic dance as the protease inhibitor targeting a particular binding site on the protease. Alternatively, we can say that the protease (more specifically, the binding site) is the target of the protease inhibitor medication. But why do medications need to have targets at all?
Drugs with Multiple Targets
Most drugs need specific targets in order to treat a particular condition. But there are indeed some drugs, like certain anti-inflammatory medications and chemotherapy treatments, that target the body as a whole. This broad approach, polypharmacology , involves one drug affecting multiple targets. Anti-inflammatory drugs reduce inflammation by acting on prostaglandins — lipids that are present all over the body. And just think of the vast array of side effects that accompany chemotherapy (fatigue, nausea, hair loss, and more). The fact a single drug causes side effects that are so different from one another, which impact different systems within the body, indicates that the drug is acting on several distinct targets.
Considering the meticulous effort that goes into seeking and identifying precise targets during the drug discovery process, it might sound surprising that scientists purposely design some medications to have many targets. But for diseases such as cancer, whose wide-ranging warpaths can span multiple organs and pose a risk to the body overall, having a less specific set of targets might be the ideal solution. Each affected organ is unique, with its own profile of cell types, enzymes, and functions. The goal here is to give patients a better chance of beating a whole-body disease with a drug whose targets live throughout the whole body.
Depending on the nature of the disease, a drug’s ability to target many molecules may be either advantageous or disadvantageous.
Drugs with One Target
Let’s face it:it’s hard to maintain this big-picture outlook when working with such tiny molecules! We saw from the protease inhibitor discussion that a single binding site in the target (and sometimes a single mutation within a single binding site) can make all the difference as to whether a medication flourishes or flounders. What muddles this problem even further is the fact that a target can have multiple domains that serve as binding sites, or two very different types of molecules could have similar binding sites that interact with the drug. How do pharmaceutical researchers make a drug that acts on one binding site of interest, while ignoring all the others?
For drugs that target only one molecule, the binding interactions between the medication and its target are extremely specific. That’s an understatement! This high specificity minimizes the risk of off-target effects that can have unpleasant or dangerous consequences on the patient’s health. Designing an effective drug that has one, and only one, target requires a deep understanding of binding affinity and the structural qualities that govern it.
Remember that the drug and the target each boast a chemical structure that’s full of functional groups. Each functional group has distinctive properties that influence its reactivity, behavior, and interactions with other molecules. This means that structural characteristics lie at the core of the drug-target binding, and therefore at the core of drug effectiveness. By manipulating the functional groups in the drug’s molecular backbone, researchers can manipulate the reactions that the drug undergoes, as well as its propensity to bond with a specific domain on the target. It’s astonishing that changing out even one little atom could introduce a different a functional group and, by extension, impact a medication’s ability to work properly! Even if the drug’s functional groups stay the same, a minor change in their spatial arrangement might completely change the medication’s function.
Consider enantiomers :molecules whose structures are mirror images. One notorious case of this chirality making or breaking a medication is thalidomide. Thalidomide is a drug that was originally marketed as a morning sickness remedy. It exists as two enantiomers:the R enantiomer has a sedative effect that alleviates symptoms like morning sickness, while the S enantiomer can cause birth defects. The only chemical difference between these two drastically different outcomes is how these molecules’ atoms are spatially arranged. To make matters worse, thalidomide can interconvert its enantiomers in vivo , so even if a patient were only administered the relatively harmless R enantiomer, the teratogenic S enantiomer may arise in the body afterwards. By contrast, medications that only exist as one enantiomer, as opposed to a racemic mixture, are enantiopure drugs.
Another example of a more-than-microscopic structural change having a larger-than-life impact is the methamphetamine molecule. Methamphetamine is a stimulant and recreational drug, with side effects like vasoconstriction and rapid breathing. Its optical isomer levmetamfetamine, meanwhile, serves as a nasal decongestant of all things! Again, we see that one small switch in these drug molecules’ atomic arrangements leads to wildly different health effects.
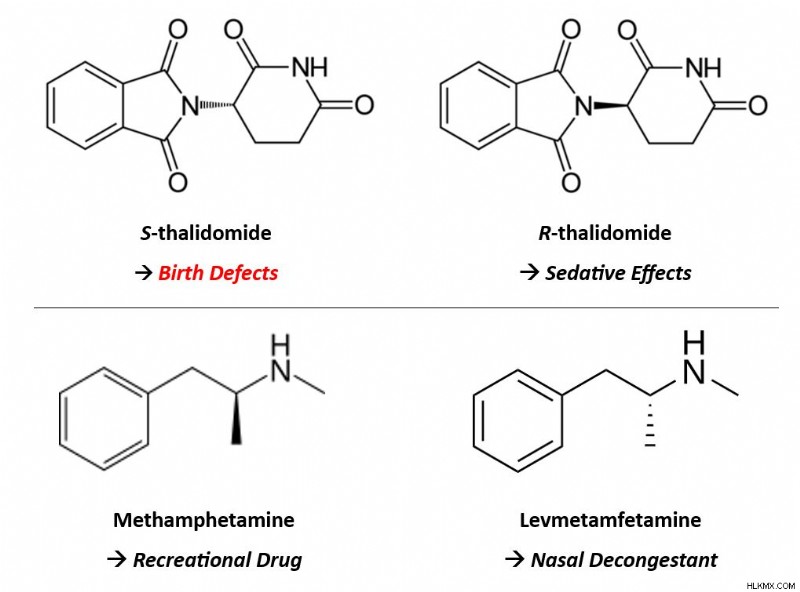 Though the only difference between each of these sets of enantiomers is the spatial arrangement of their atoms, their ensuing medical effects differ greatly.
Though the only difference between each of these sets of enantiomers is the spatial arrangement of their atoms, their ensuing medical effects differ greatly. A recurring notion in drug development is that medications are intended to be as safe and effective as possible. However, no medication can be 100% safe nor 100% effective. No matter what, there’s always the risk of side effects, off-target effects, and unwanted interactions. Regardless, scientists can maximize safety and effectiveness by tailoring a drug’s chemical properties, like its structure and functional groups, to be as specific as possible to the target of interest.
Unfortunately, achieving that specificity can be an intense challenge, especially when only one target is desired. But when different pathogens employ the same biochemical processes or enzymes as each other — like how SARS-CoV-2, HIV-1, and hepatitis C virus all employ proteases for replication — these features serve as a good starting point for drug design. Could that common feature potentially function as the drug’s target? And since several pathogens share that feature, could the drug therefore be effective against all of the pathogens? For viruses in particular, all viruses must replicate because replication is the only way viral diseases can spread to new hosts. That’s why popular COVID-19 medications target molecules, like proteases, that have a central role in SARS-CoV-2 replication. (The same is true for the protease inhibitor drugs that treat HIV and hepatitis C infection.)
Here, we’ve seen that slight changes in the drug molecule yield big impacts on its ability to bind selectively with its target (or targets). Later, we’ll talk about another highly-specific mechanism in combating disease:the interactions between antibodies and antigens. For now, let’s dive into the question of why COVID-19 medications were unusually difficult to make.
Drug Development under Dire Circumstances
The small but significant principles that we’ve mentioned so far — the fact that antibiotics don’t work against viruses, the puzzle of creating a new medication based on clues from existing ones, the arduous task of designing a drug with meaningful targets — only complicated the hunt for efficacious COVID-19 medications. Numerous additional factors were already at play, presenting challenges for drug development during a time when we needed it most.
Some of these challenges ran deep. Hardening travel restrictions and heightened political tensions, for example, strained the pharmaceutical supply chain at its core. Patients often rely on drugs manufactured elsewhere in the world, but temporary limits on international travel jeopardized typical medication supply. Worth noting is that most active pharmaceutical ingredients (APIs ), the component of a drug that gives it its therapeutic effect, are manufactured outside of the U.S. This includes being manufactured in countries that the pandemic hit hard, such as China. Importing drugs and APIs — and exporting American medicines to patients around the world — normally happens in a steady stream that ensures patients everywhere can receive their treatments when they expect to. With the short-term closures of pharmaceutical facilities and chemical plants domestically and abroad, this promise went unfulfilled in many cases. Even a brief pause in drug manufacturing can ripple into long-lasting consequences for patients.
 Pandemic-related travel restrictions hindered international drug distribution, preventing some medicines from reaching patients when expected.
Pandemic-related travel restrictions hindered international drug distribution, preventing some medicines from reaching patients when expected. Other points in the drug development process were interrupted, too. The Food and Drug Administration (FDA ), the American pharmaceutical regulatory agency, also monitors pharmaceutical sites in foreign countries. These inspections confirm that U.S.-bound drugs comply with the same rigorous safety and quality standards as those made in America. International travel restrictions, again, delayed these investigations. Inspections must happen before any medications get distributed, so from a patient perspective, postponed inspections equates to postponed treatment.
The COVID-19 pandemic struck all steps in the pharmaceutical supply chain:manufacturing, production, approval, distribution, and everything in between. This highlighted glaring vulnerabilities in this industry’s very framework, and those vulnerabilities’ effects on patients. We expect pandemics to arise occasionally, but we can’t predict when, and no two disease outbreaks are the same. That aspect of “unexpectedness” makes it extra hard to accommodate them when they do happen. Even more urgently, it underscores the need to make our drug development processes more resilient against health emergencies like pandemics. Let’s take a moment to see what that impact looks like in the context of pharmaceutical research.
A Logistical Nightmare
As soon as the World Health Organization classed COVID-19 as a pandemic, the clinical research sector scrambled to accommodate this. Mounting concerns over a mysterious disease abruptly brought many clinical trials to an indefinite pause. By the time a clinical trial starts, the researchers have already carefully planned and committed to its study protocol. During COVID-19, social distancing guidelines forced them to reimagine studies in virtual formats when possible, and postpone them when not. Trials that hadn’t begun yet were hit even harder. The number of prospective study participants plummeted as they feared COVID-19 exposure in the medical facilities where trials often occur. Some studies couldn’t even get off the ground, but those that could suddenly found themselves stuck in midair.
What’s the problem with putting a clinical trial on pause? It’s not as simple as picking up where the study left off a few weeks afterward. Surprisingly, a lot can happen in the span of a few weeks. If study participants have already received a trial dose of the drug candidate, they might experience new side effects. Researchers need to monitor these complications closely to document and address them, and to ensure the drug’s safety. Ongoing communication is paramount during trials by ensuring patients understand the nature of the study and can express their concerns. Anything that interferes with these open lines of communication, like a brutal pandemic, potentially puts the patient’s safety at risk.
During this frantic period, coronavirus clinical trials took center stage as new COVID-19 medications, therapeutics, and vaccines evolved. A large portion of biomedical research funding, media attention, and public health efforts were diverted to these studies. There’s nothing inherently bad about this, but COVID-19 wasn’t the only disease that needed trials at the time. Pausing routine studies in favor of COVID-19 trials means neglecting, at least temporarily, patients who have other medical conditions. The timing was unlucky, but other diseases didn’t cease to exist just because the pandemic happened. Striking this balance given a wide pool of patients in need, and redirecting funding appropriately, was a big challenge as COVID-19 cases skyrocketed. It even represents complex bioethical questions:How “worth pursuing” is a particular disease compared to others? Is it even possible to “rank” the value of different diseases? Who gets to determine this value?
Among the most unsettling outcomes of the pandemic is that it brought our health care infrastructure’s flaws to light. Many individuals, especially practitioners and patients who experience the health care system firsthand, were already acutely aware of its shortcomings. But COVID-19 exposed these imperfections and made them impossible to ignore. Already stretched thin, medical staff and facilities didn’t have adequate support or resources during intense waves of COVID-19 variants. Issues surrounding health equity, like overcoming health disparities and ensuring accessibility to drug treatments, became serious problems for some patients. These problems predated COVID-19 and aren’t unique to it, but the pandemic certainly emphasized them. As we determine a path forward in a post-pandemic world, public health experts think deeply about how to solve problems like these, to help everyone pursue their healthiest self.
 Resolving a pandemic extends beyond drug development. Health care personnel, regulatory employees, policymakers, and public health experts each have a key role in coordinating an effective pandemic response.
Resolving a pandemic extends beyond drug development. Health care personnel, regulatory employees, policymakers, and public health experts each have a key role in coordinating an effective pandemic response. The COVID-19 Treatment Toolbox
So far, we’ve covered two types of antiviral COVID-19 medications in detail. That’s not the whole story, though. There are other COVID-19 antiviral drugs too, and pharmaceutical treatments aren’t limited to pills either. In this section, we’ll see how the pandemic employed a multitude of other forms of treatment, even making use of the body’s natural defense mechanisms.
Monoclonal Antibodies
Even when it’s combating an infection like COVID-19, the immune system is a very powerful force. A relentless soldier in the battle for your health, its most intrinsic mission is to protect you, and it’s determined not to give up. To achieve this goal, the immune system utilizes its diverse range of physiological intricacies, some of which researchers don’t fully understand yet. Immunologists do understand the basic mechanism of how it works, though.
When a foreign pathogen, like the SARS-CoV-2 virus, infects you, we call that pathogen an antigen . The immune system recognizes antigens as invaders and mounts an immune response to ambush them. Among other biochemical battalions, it deploys antibodies. Antibodies are proteins made by the body’s B cells that selectively bind to antigens like a key fitting a lock. Binding is a way of flagging the antigen so other immune cells can identify, attack, and neutralize or kill it. As a component in pharmaceutical treatments, antibody therapy is an auspicious option for patients whose bodies can’t mount a sufficient immune response on their own.
How do monoclonal antibodies work?
We can classify antibodies into two broad categories. Monoclonal antibodies (mAbs ) are antibodies that target a single antigen. They’re man-made in the lab by cloning a single lineage of B cells, hence the name. By contrast, polyclonal antibodies (pAbs ) derive from multiple immune cells, arise naturally in the body in response to an infection, and can target multiple antigens.
We usually discuss mAbs as an immunotherapy in the context of cancer, where the “antigen” that they recognize is a protein on the surface of a cancer cell. More recently, their applications have extended to other conditions, including COVID-19. (Another pharmaceutical lingo lesson:a drug whose generic name ends in “-mab” is a type of monoclonal antibody.) When administered to patients, mAbs stimulate the immune system and can improve their chances of fighting off an infection. Creating mAbs in laboratories is an opportunity to precisely tailor them to a specific condition, which can enhance patient outcomes. Pharmaceutical scientists can mass-produce them with high consistency, and off-target effects are relatively unlikely because the mAb binds to only one antigen.
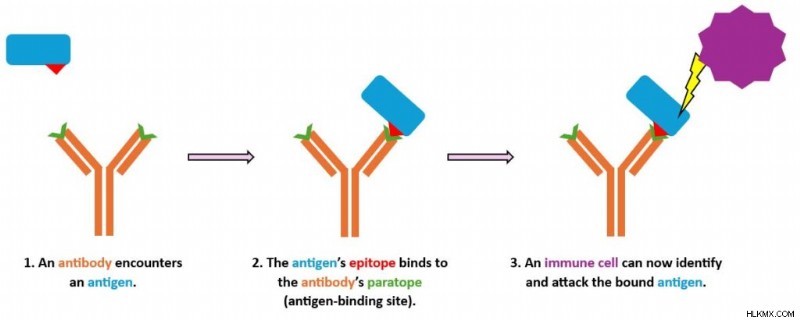
How does that binding make the magic happen? Given its Y-like shape, an antibody has two arms that branch off from its body (the Y’s vertical stem). On the end of each arm is a paratope , the region that binds directly to an antigen. The antigen itself features a region called an epitope . The antibody’s paratope and antigen’s epitope are extremely specific to each other. Consequently, the molecules bind together in a selective and precise manner, like a lock and key. Once the antibody has latched on to the antigen, the immune system can take action to attack that antigen.
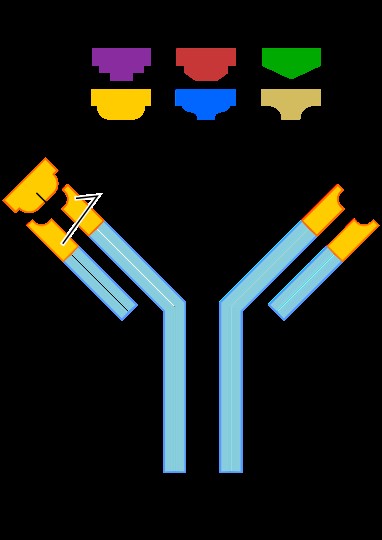 Antigens come in all shapes and sizes, but only a specific antigen can bind to a given antibody’s antigen-binding site (paratope).
Antigens come in all shapes and sizes, but only a specific antigen can bind to a given antibody’s antigen-binding site (paratope). Over time, researchers have found that COVID-19 mAbs can have different levels of effectiveness against certain SARS-CoV-2 variants. COVID-19 mAbs tend to have a harder time fighting off recent variants compared to older ones. As the pandemic evolved, novel variants dominated new infections, and some variants even showed resistance against COVID-19 treatments. It quickly became evident that antibody therapy alone, though a valuable aid, wouldn’t be a long-term solution to COVID-19.
Newly-produced antibodies travel from the B cell (a white blood cell) to the antigen’s location via the patient’s blood plasma. Everyone has blood plasma, but COVID-19 patients may be able to supplement their treatment with convalescent plasma. Next, we’ll see what that means and why it matters.
Convalescent Plasma
We just described how an infection engages the body’s immune response, including increasing the amount of antibodies in the blood. We also mentioned that the immune system’s B cells naturally produce polyclonal antibodies during an infection.
In patients who survive the infection, those antibodies don’t disappear after their symptoms clear up. As the infection resolves, the antigens in the body dwindle. But just in case these antigens dare to show their face around these parts again (in other words, if the patient were to contract the virus again in the future), these antibodies remain in the body, lying in wait to flag them for removal.
Therefore, people who have survived COVID-19 still have COVID-19 antibodies in their blood plasma. Plasma is the part of blood that excludes blood cells and platelets. Survivors can donate this blood plasma, and HCPs then process it and transfuse it into the veins of patients who are actively sick. This was a big deal during the first phase of the pandemic, before researchers managed to make a vaccine that teaches the body’s immune system to create COVID-19 antibodies. And once the vaccines were available, vaccinated folks could donate their antibody-rich plasma to COVID-19 patients even if they’d never actually had an infection themselves.
 Donor blood processing removes components like red blood cells, which is why plasma isn’t red in color.
Donor blood processing removes components like red blood cells, which is why plasma isn’t red in color. Plasma therapy is viable particularly for immunocompromised patients, who may not be capable of launching robust immune responses without it. It’s a great way for COVID-19 survivors to pay it forward and play a personal role in helping current patients. Plasma therapy is useful due to its potential to shorten the duration or severity of infection. In 2020, when no feasible COVID-19 medications were available, having ready-made antibodies in our arsenal was practical and priceless.
Making the Most of COVID-19 Medications
Antibody therapy and plasma therapy are two non-antiviral tools that HCPs relied upon during the worst waves of the pandemic. Once COVID-19 medications hit the market, they became the go-to treatment for active infections because they successfully interrupt the viral life cycle. But if you find yourself infected with COVID-19, the medication that suits your needs might depend on factors like your age and risk of hospitalization. Each of these drugs works most effectively when taken shortly after the onset of symptoms. Why does when you take the medicine matter? It’s ideal to intervene during the initial stages of infection, before the virus has extra time to damage the body. This is especially important in severe cases, when such damage could be extensive.
As is the case with other viral infections, prioritizing rest and fluid intake can go a long way in COVID-19 recovery. In more severe cases, supplemental oxygen and around-the-clock care might be necessary to help hospitalized patients heal. Without innovative antivirals around yet, early waves of the pandemic relied heavily on supportive care techniques like these. Now approved by regulatory authorities, drugs like nirmatrelvir/ritonavir are quite accessible, as long as you have an HCP’s prescription. They’ve even surpassed supportive treatments and taken center stage as the first line of defense against an active COVID-19 infection due to their efficacy and reliability. Nonetheless, HCPs can use all of these treatment types in tandem to make their combined impact more effective.
Despite all of their advantages, antiviral drugs don’t replace other infection control tactics. Patients using COVID-19 medications are still advised to self-isolate until their infection resolves or, if that’s not an option, wear a mask and practice social distancing. Here, let’s also note that these medications only treat existing cases; they don’t do anything to protect patients against future COVID-19 infection. Instead, those prevention measures are best addressed using vaccines and prophylaxis, two tactics we’ll explore later in this mini-series, as well as old school strategies like good hand hygiene. The classics never go out of style!
결론
The worst of the COVID-19 pandemic has now passed, but epidemiology demonstrates the constant skirmish between the scientific tools underlying public health and the increasing fortitude of formidable pathogens. As we anticipate future pandemics, we can plan ahead by reflecting on our past successes and shortfalls, and now we have effective treatments in case new COVID-19 cases recur in the future. These treatments, though challenging to invent and deploy, represent a great achievement in the biomedical research realm. Although we can’t fully cure viral infections, the good news is that we can prevent them. In a forthcoming article in this public health mini-series, we’ll explore the advanced array of preventive measures — including the groundbreaking mRNA vaccine technology — that stopped COVID-19’s spread in its tracks.
What happens in the body between the time patients are prescribed COVID-19 medications and the time they start to feel better?